

IT Band pain while running? Why is it happening and how do you fix it?
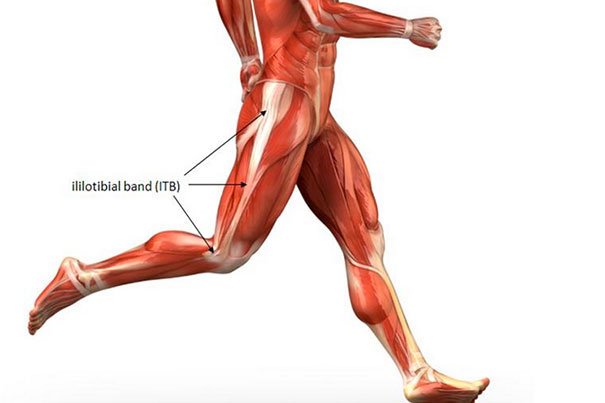
The most common site of pain I’ve come across in runners this spring and summer is at the iliotibial band (ITB). Generally this presents as pain at outside of the knee but can also show up as pain around the hip. The ITB is a very sturdy fascial structure running from the crest of your hip, along the side of your thigh to the tibia.
Traditionally I see pain at this area when training load is ramped up too quickly and/or new trail or terrain is added into your plan. I do not see these variables as the root cause of pain but they do not help our cause. From a movement quality perspective I see a few faults show up in most patients with ITB irritation.
1. Pelvic drop, this is the most common issue runners with ITB pain face. When describing pelvic drop, I am referencing your belt line. When in single limb stance your belt line should be level to the ground, in a perfect world. When we can visualize that belt line dropping significantly we starting thinking of glute med/min referral pain or ITB irritation. This can be a bit tough to determine if you are doing this yourself while running but with a simple step down test in a mirror you may see yourself dropping the hip. Most of our clients who have pelvic drop in a step down test also show excessive drop at mid stance when running.

In the runner above you can note a pelvic drop of 5.8 degrees. This amount of drop would cause some concern. As the pelvic angle increases we should expect lateral thigh irritation and possible symptoms related to lack of active shock absorption.
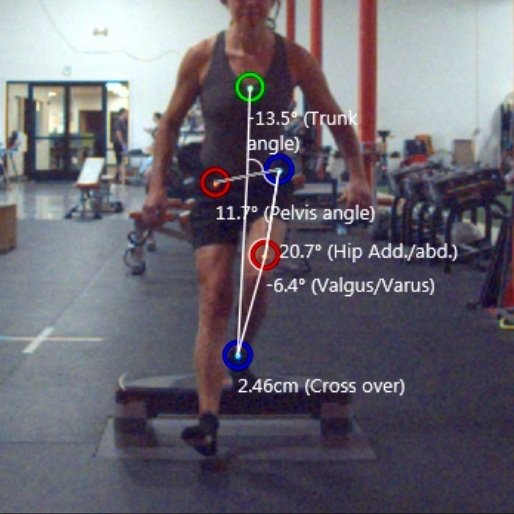
If you do not have a good way to film yourself while running to determine if you are dropping the pelvis too much a simple step down in a mirror at home can be quite helpful. In the image above you will note this runner is showing a pelvic drop angle of 11.7 degrees. This would be considered excessive and most likely, a large contributor to her ITB pain. When we see this type of pelvic drop in mid stance while running or during a step down we focus on treatment strategy around glute medius. This muscle is laterally aligned on the hip and is a strong hip abductor. Meaning, when strong/active, the glute medius will control the pelvis angle quite well.
2. Dynamic knee valgus is another common movement fault seen in runners experiencing ITB pain. This fault is characterized by the knee collapsing inward toward midline. Primarily comprised of internal rotation of the femur, knee valgus should be controlled by glute maximus activation during the gait cycle. Knee valgus collapse combined with pelvic drop during stance phase of running is a likely cause of the ITB to be irritated. In this scenario the ITB is tensioned very aggressively in the energy absorption phases of gait. With enough repetition this can be enough to cause injury and inflammation at the ITB itself.
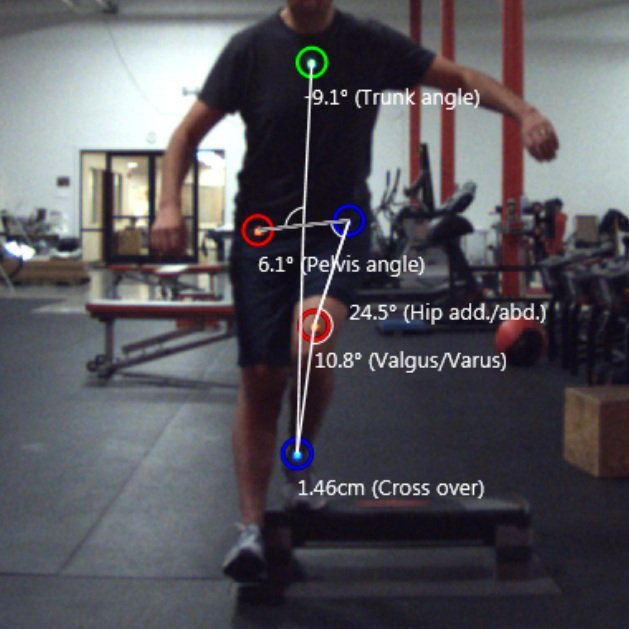
In the runner seen above, a combination of pelvic drop around 6 degrees and dynamic knee valgus around 11 degrees would be considered problematic. Our primary treatment strategy here will be to activate the glute max and med throughout the gait cycle.
3. The third most common fault seen in runners who experience ITB pain is a lack of hip extension mobility. Hip extension is when the femur move backward behind you in the swing phase of gait. I look for our athletes to have a true 15 degrees of extension passively. Almost all of the patients I see for lower extremity pain complaints lack hip extension t show extent. This lack of mobility can cause a host of issues up and down the body. Primarily I see a lack of access to the glute musculature along with hip extension restriction. I also see overextension at the lumbar spine in swing in folks that are limited in hip extension.

In the images above it may be a bit difficult to visualize the lack of hip extension in this athlete as it does seem that her femur is moving backward in push off and flight phases. We like to assess this range of motion with a neutral pelvic position. Meaning her belt line should be level to the ground for the most accurate measurement of hip extension. In these images her pelvis is rotated anteriorly and in turn she is achieving her hip mobility through a combination of hip motion and lumbar spine over extension.
So, excessive pelvic drop, excessive dynamic knee valgus and a lack of hip extension may be directly related to your ITB pain. What should you start working on now?
Practicing single leg squats are a great way to focus on maintaining a level belt and keeping your knee aligned over your foot and ankle.
Split squats with band resistance provide should remind your to maintain good external rotation torque at the femur via firing your glute max. Focus on rotating the entire leg outward so the knee is on top of the foot, not inside.
Fire hydrants are excellent at activating the glute max and skaters are excellent are activating the glute med. I like to start with static holds and follow that up with repetitions.
This stretch is a great way to open up the anterior hip and allow the femur to move behind you more easily. Focus should be on tucking the tail while keeping the trunk tail. Gentle holds for a long duration are ideal.
Add in some extra rolling for the glute muscles you just worked on. I prefer rolling side to side vs up and down for trigger point release work.